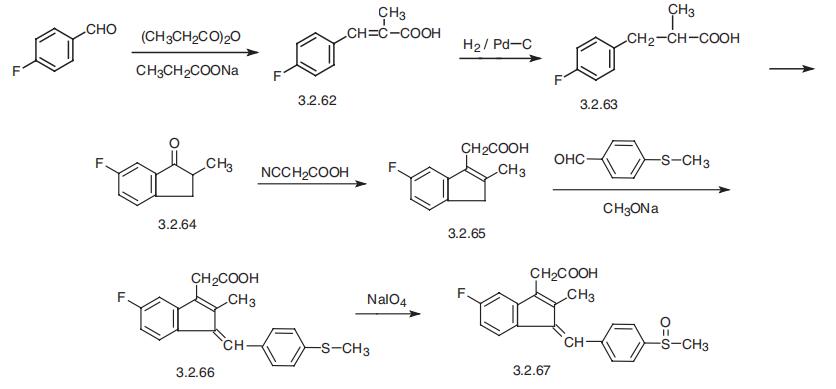
Sulindac
- Product NameSulindac
- CAS38194-50-2
- MFC20H17FO3S
- MW356.41
- EINECS253-819-2
- MOL File38194-50-2.mol
Chemical Properties
| Melting point | 182-185°C |
| Boiling point | 581.6±50.0 °C(Predicted) |
| Density | 1.2581 (estimate) |
| storage temp. | Sealed in dry,Store in freezer, under -20°C |
| solubility | Very slightly soluble in water, soluble in methylene chloride, sparingly soluble in ethanol (96 per cent). It dissolves in dilute solutions of alkali hydroxides. |
| form | Solid |
| pka | pKa (25°) 4.7 |
| color | Light yellow to Brown |
| biological source | synthetic (organic) |
| Water Solubility | Soluble in water, methanol, ethanol. |
| λmax | 327nm(0.05mol/L methanolic HCl)(lit.) |
| Merck | 14,8982 |
| Major Application | forensics and toxicology veterinary |
| Cosmetics Ingredients Functions | ANTIOXIDANT |
| InChI | 1S/C20H17FO3S/c1-12-17(9-13-3-6-15(7-4-13)25(2)24)16-8-5-14(21)10-19(16)18(12)11-20(22)23/h3-10H,11H2,1-2H3,(H,22,23)/b17-9- |
| InChIKey | MLKXDPUZXIRXEP-MFOYZWKCSA-N |
| SMILES | CC1=C(CC(O)=O)c2cc(F)ccc2\C1=C/c3ccc(cc3)S(C)=O |
| CAS DataBase Reference | 38194-50-2(CAS DataBase Reference) |
Safety Information
| Hazard Codes | Xn |
| Risk Statements | 22-63-42/43 |
| Safety Statements | - |
| RIDADR | 3249 |
| WGK Germany | 3 |
| RTECS | NK8226000 |
| HazardClass | 6.1(b) |
| PackingGroup | III |
| HS Code | 29309090 |
| Storage Class | 6.1C - Combustible acute toxic Cat.3 toxic compounds or compounds which causing chronic effects |
| Hazard Classifications | Acute Tox. 3 Oral Repr. 2 Resp. Sens. 1 Skin Sens. 1 |