Faropenem: Antimicrobial Activity, Susceptibility, Toxicity and Clinical Uses
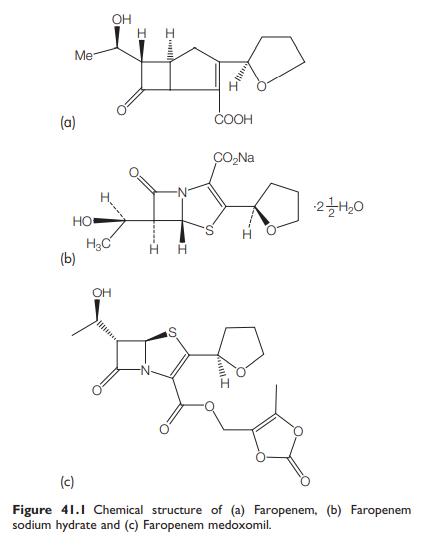
Faropenem is a penem-class oral b-lactam antimicrobial agent. Although faropenem is structurally similar to the carbapenems, it is distinguished by a sulphur atom at position 1. In Japan, faropenem has been available since 1997 as faropenem sodium hydrate (Faroms), whereas in the USA, faropenem is in phase III clinical trials as the ester prodrug, faropenem medoxomil (also known as faropenem daloxate) (Schurek et al., 2007; Gettig et al., 2008). Faropenem is notable because it is one of the few carbapenem-like agents that can be given orally.
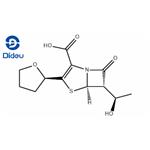
Faropenem is effective against common community-acquired pathogens, such as Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, methicillin-susceptible Staphylococcus aureus (MSSA), other streptococci, E. coli, and anaerobes. However, faropenem is not active against methicillin-resistant S. aureus (MRSA), Enterococcus faecium, Pseudomonas aeruginosa, and Stenotrophomonas maltophilia, and it tends to show relatively high MICs to Enterococcus faecalis and some Enterobacteriaceae. Faropenem has bactericidal activity by way of its interaction with penicillin-binding proteins (PBPs) like all other b-lactam antibiotics (Schurek et al., 2007). The chemical structures of faropenem, faropenem sodium hydrate, and faropenem medoxomil are shown in Figure 41.1.

Figure 41.1 Chemical structure of (a) Faropenem, (b) Faropenem
sodium hydrate and (c) Faropenem medoxomil.
ANTIMICROBIAL ACTIVITY
a. Routine susceptibility
A summary of the in vitro activity of faropenem is shown in Tables 41.1
and 41.2.
Gram-positive bacteria
Faropenem is quite active against the major pathogens of communityacquired respiratory infections, including Streptococcus pneumoniae. Most strains of S. pneumoniae are highly sensitive to faropenem, although the MICs of faropenem for penicillin-intermediate and resistant strains are higher than those for penicillin-susceptible strains (Milatovic et al., 2002; Decousser et al., 2003; Critchley et al., 2007). Faropenem is highly active against streptococci other than pneumococci and MSSA. Enterococcus faecalis is less sensitive to faropenem, and E. faecium and MRSA are resistant (Milatovic et al., 2002).
Gram-negative bacteria
Haemophilus influenzae and Morganella catarrhalis are sensitive, and
there are no significant differences in faropenem MICs between blactamase-
positive and -negative strains (Milatovic et al., 2002;
Schmitz et al., 2002; Walsh et al., 2003; Sanbongi et al., 2006;
Critchley et al., 2007). Faropenem has good activity against Escherichia
coli, Klebsiella pneumoniae, and K. oxytoca. However, the other
Enterobacteriaceae, such as Citrobacter freundii, Enterobacter spp., M.
morganii, Proteus spp., Providencia spp., and Serratia spp. are less
sensitive to faropenem (Milatovic et al., 2002).
Table 41.1 In vitro susceptibility of selected Gram-positive bacteria to faropenem.
MECHANISM OF DRUG ACTION
The activity of faropenem against bacteria is determined by its binding
to PBPs as with other b-lactams. Dalhoff et al. (2003b) studied the
affinity of faropenem to various PBPs in S. aureus, E. coli, P. vulgaris,
P. aeruginosa, S. marcescens, S. pneumoniae, and E. faecalis. Faropenem exhibited higher affinity to the high molecular weight PBPs (PBP1, 2,
and 3) than to the low molecular weight PBPs (PBP4, 5, and 6) in
most bacteria, with the exception of P. vulgaris,
S. marcescens, and E. faecalis (Dalhoff et al., 2003b).
MODE OF DRUG ADMINISTRATION AND DOSAGE
a. Adults
In randomized trials of faropenem medoxomil which have been performed in the USA, Canada, Latin America, Europe, and South Africa, a dose of 300 mg twice-daily orally has been employed. In Japan, a dose of 200–300 mg twice or three times daily orally of faropenem sodium is approved by the Pharmaceutical and Medical Devices Agency (PMDA).
b. Newborn infants and children
There have been no published data of faropenem medoxomil in the treatment of infectious diseases of newborn infants and children. In Japan, a dose of 5–10 mg/kg three times daily p.o. (not exceeding 300 mg at one time or 900 mg/day) of faropenem sodium is approved for the use in pediatric patients by the PMDA. There has been no experience for faropenem sodium or faropenem medoxomil in premature neonates.

Table 41.2 In vitro susceptibility of selected Gram negative bacteria to faropenem.
TOXICITY
a. Gastrointestinal adverse events
The most common adverse events during treatments by faropenem are gastrointestinal, such as diarrhea, nausea, and vomiting. However, the frequency of those events (15%) was similar to the comparators, including penicillin, amoxicillin, amoxicillin–clavulanate, cephalexin, cefuroxime axetil, cefpodoxime, clarithromycin, azithromycin, and TMP-SMX (Schurek et al., 2007).
b. Hypersensitivity reactions
The frequency of hypersensitivity reactions to faropenem medoxomil or faropenem sodium is not yet clear. Cross-reactivity of faropenem to other b-lactams, such as penicillin, is possible, but its frequency has not been defined.
c. Fetal toxicity
There are no data in humans regarding fetal toxicity, but animal experiments show no teratogenicity (Maruho, 2008).
CLINICAL USES OF THE DRUG
a. Acute bacterial sinusitis
A prospective, double-blind, multicenter trial compared faropenem medoxomil 300 mg twice-daily for 7 days with cefuroxime axetil 250 mg twice-daily for 7 days for the treatment of acute bacterial sinusitis (Siegert et al., 2003). Clinical cure rate and bacteriologic success rates at day 7 were similar for faropenem medoxomil and cefuroxime axetil.
b. Community-acquired pneumonia
A multicenter noninferiority trial conducted in Europe, Latin America, and South Africa compared the safety and efficacy of faropenem medoxomil and amoxicillin in the treatment of communityacquired pneumonia. Patients were randomized to receive either faropenem medoxomil 300 mg twice-daily for 10 days or amoxicillin 1000 mg three times daily for 10 days. This study showed that faropenem was noninferior to amoxicillin for the treatment of community-acquired pneumonia (Kowalsky et al., 2005; Gettig et al., 2008).
c. Acute exacerbation of chronic bronchitis
Two multicenter noninferiority trials have demonstrated the safety of faropenem in acute exacerbation of chronic bronchitis (Gettig et al., 2008). Faropenem has not been compared with placebo, to unequivocally demonstrate efficacy.
d. Uncomplicated skin and skin-structure infection
Faropenem medoxomil was compared with amoxicillin–clavulanate in the treatment of uncomplicated skin and skin-structure infections in a noninferiority trial (Corrado and Echols, 2005; Gettig et al., 2008).
References
Boswell FJ, Andrews JM, Wise R (1997). Pharmacodynamic properties of
faropenem demonstrated by studies of time kill kinetics and postantibiotic
effect. J Antimicrob Chemother 39: 415.
Boswell FJ, Ashby JP, Andrew JM, Wise R (2002). Effect of protein binding on
the in vitro activity and pharmacodynamics of faropenem. J Antimicrob
Chemother 50: 525.
Decousser JW, Pina P, Picot F, Allouch PY (2003). Comparative in vitro activity
of faropenem and 11 other antimicrobial agents against 250 invasive
Streptococcus pneumoniae isolates from France. Eur J Clin Microbiol Infect Dis
22: 561.
Gettig JP, Crank CW, Philbrick AH (2008). Faropenem medoxomil. Ann
Pharmacother 42: 80.
Hiraga N, Muratani T, Naito S, Matsumoto M (2008). Genetic analysis of
faropenem-resistant Enterococcus faecalis in urinary isolates. J Antibiot 61:
213.
Jones RN, Critchley IA, Whittington WL et al. (2005). Activity of faropenem
tested against Neisseria gonorrhoeae isolates including fluoroquinoloneresistant
strains. Diag Microbiol Infect Dis 53: 311.
Mushtaq S, Hope R, Warner M, Livermore DM (2007). Activity of faropenem
against cephalosporin-resistant Enterobacteriaceae. J Antimicrob Chemother
59: 1025.
Okamoto K, Gotoh N, Nishino T (2001). Pseudomonas aeruginosa reveals high
intrinsic resistance to penem antibiotics: Penem resistance mechanisms and
their interplay. Antimicrob Agents Chemother 45: 1964.
Sanbongi Y, Suzuki T, Osaki Y et al. (2006). Molecular evolution of b-lactamresistant
Haemophilus influenzae: 9-year surveillance of penicillin-binding
protein 3 mutations in isolates from Japan. Antimicrob Agents Chemother 50:
2487.
Woodcock JM, Andrews JM, Brenwald NP et al. (1997). The in-vitro activity of
faropenem, a novel oral penem. J Antimicrob Chemother 39: 35.
You may like
Related articles And Qustion
Lastest Price from Faropenem manufacturers
US $0.00-0.00/KG2025-11-18
- CAS:
- 106560-14-9
- Min. Order:
- 1KG
- Purity:
- 98
- Supply Ability:
- 10000KGS