Vardenafil: pharmacodynamic properties, mechanism of action, dosage and Administration
Introduction
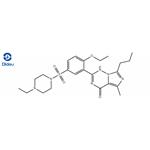
Vardenafil (Figure.1) is a potent and highly selective inhibitor of cGMP-specific phosphodiesterase type 5 (PDE-5), the most prominent PDE in the penile corpus cavernosum. It has been proven to be safe and effective treatment for erectile dysfunction (ED). This action can result in smooth muscle relaxation that is needed for a penile erection . Vardenafil is 5–10 times more potent than sildenafil, the classic PDE-5 inhibitor.The drug is generally well tolerated, with a favorable safety profile. Its use is associated with few treatment-related side effects, most notably headache,flushing, indigestion and nasal congestion. Vardenafil has a rapid onset of action, and ED patients can gain erections sufficiently rigid for eventual intercourse completion as early as 10–15 min after drug intake. It is hepatically metabolized into more than 14 metabolites, the most important of which is N-desethyl vardenafil (M1). Interestingly, this metabolite is pharmacologically active.[1]

Physical properties[1]
Physical properties are as follows. Appearance: White crystalline powder;Water solubility: 0.11 mg/mL (HCl salt);Melting point: 241℃, 192℃ (free base), 214–216℃, 224–239℃. Stability: 30℃/75% relative humidity. Dissociation constant: pKa1=4.72; pKa2=6.21 (tertiary amine)/estimated (free base). Partition coefficient: P is the partition coefficient of the molecule in the water–octanol system log P: 2.65; log P: 1.4 (free base).
Pharmacodynamic Properties
Like other drugs in its class, vardenafil is a selective inhibitor of PDE5 and the in vitro activity of vardenafil has been compared with that of sildenafil. The concentration of vardenafil which inhibited 50% of the activity (IC50) of isolatedPDE5 was 0.7 nmol/L compared with 6.6 nmol/L for sildenafil, approximately a 10-fold difference. The effect of the two drugs on isoforms of PDE was also determined. For vardenafil versus sildenafil the IC50 values in nmol/L were 180 vs 396 (PDE1), >10 000 vs >10 000 (PDE2), 2 500 vs17 000 (PDE3), 4 000 vs 12 000 (PDE4) and 11 vs49 (PDE6).[2]
Vardenafil is a safe and well-tolerated treatment of men with ED. It is a highly potent and selective inhibitor of PDE-5, the most prevalent phosphodiesterase in the human penile corpus cavernosum, and thus increases intracellular cGMP levels in the cavernosum tissue of the penis. It was the first second-generation PDE-5 inhibitor that received marketing approval in the United States. Unlike the other PDE-5 inhibitors, sildenafil and tadalafil, Vardenafil was developed from the outset specifically for use as an erectogenic agent. It is 5–10 times more potent than sildenafil, the classic PDE-5 inhibitor. Vardenafil has been shown to be efficacious in the treatment of ED in the doses of 10 and 20 mg taken on demand, prior to intercourse. For most patients, the recommended starting dose is10 mg, which according to US labeling information should be taken approximately 60 min prior to sexual activity. Adverse effects associated with Vardenafil are not severe, mostly dose dependent and tend to decrease with time. These include headache, flushing, dyspepsia, and rhinitis.[1]
Mechanism of action
Vardenafil increases penile rigidity and tumescence via a mechanism of action similar to that of the other PDE-5 inhibitors, sildenafil and tadalafil. It facilitates penile erection by the inhibition of cGMP-specific PDE-5, the most active PDE involved in the termination of cGMP signaling in the penile corpus cavernosum, the erectile tissue in the penis. This, in turn, potentiates endogenous increases in cGMP levels in the corpus cavernosum and the vessels supplying it, thus increasing dilatation of the corporeal sinusoids allowing more blood flow, which induces an erection. Interestingly, this occurs only in the presence of nitric oxide release with sexual arousal. Sexual stimulation causes the release of nitric oxide (NO) from neurons and endothelial cells in the corpus cavernosum. NO, in turn, activates the enzyme guanylyl cyclase, with the resultant conversion of guanosine triphosphate to cGMP. This results in activation of cGMP-dependent protein kinase,phosphorylation of several proteins and reduction of intracellular calcium levels, and a consequent smooth muscle relaxation and an increased arterial blood flow leading to enlargement of the corpus cavernosum. Because of the increased tumescence, veins are compressed between the corpus cavernosum and the tunica albuginea, leading to an erection. Notably, Vardenafil has no effect on NO release and is, thus, ineffective in causing erection in the absence of sexual arousal.[1]
Dosage and Administration
Vardenafil is approved in the US and the EU for the treatment of ED. The recommended dose of vardenafil in adult men is 10mg; however, the dose may beincreased to the maximum recommended dose (20mg) or decreased to 5mgaccording to efficacy and tolerability. It is recommended that vardenafil not betaken more than once daily. Vardenafil should be taken orally prior to sexual intercourse. Vardenafil is not indicated for use in women or in individuals aged<18 years.[3]
Metabolism and Elimination
Vardenafil is predominantly metabolised by cytochrome P450 (CYP)3A4; CYP3A5 and CYP2C also contribute to the metabolism of the drug. Desethylation of vardenafil results in Ml (the major circulating metabolite). Ml is pharmacologically active with an estimated efficacy contribution of≈7%. The mean t1/2 of vardenafil 10-40mg ranged from 3.94-4.79 hours in men (aged 22-59 years) with ED. Vardenafil has a total body clearance of 56 L/h. The mean renal clearance of vardenafil was 2.3 L/h in healthy volunteers (aged 30-60 years) who received a single dose of vardenafil 20mg. Approximately 91-95% of the administered vardenafil dose is excreted as metabolites infaeces and ≈2-6% is excreted as metabolites in theurine.[3]
Tolerability
Vardenafil was generally well tolerated in men with ED. Treatment-emergent adverse events were generally of mild to moderate intensity and transient in nature.[3]
References
1. Ashour AE, Rahman AF, Kassem MG. Vardenafil dihydrochloride. Profiles Drug Subst Excip Relat Methodol. 2014;39:515-544. doi:10.1016/B978-0-12-800173-8.00009-X
2. Ormrod D, Easthope SE, Figgitt DP. Vardenafil. Drugs Aging. 2002;19(3):217-229. doi:10.2165/00002512-200219030-00005
3. Keating GM, Scott LJ. Vardenafil: a review of its use in erectile dysfunction. Drugs. 2003;63(23):2673-2703. doi:10.2165/00003495-200363230-00010
You may like


Lastest Price from Vardenafil manufacturers
US $0.00-0.00/KG2025-12-15
- CAS:
- 224785-90-4
- Min. Order:
- 1KG
- Purity:
- 98
- Supply Ability:
- 10000KGS
US $0.00/kg2025-08-29
- CAS:
- 224785-90-4
- Min. Order:
- 1kg
- Purity:
- 99.0%
- Supply Ability:
- 1000kg