Nicotinic Acid: Mechanism of Action, Effect on Lipid Profile and Cardiovascular Risk
General Description
Nicotinic acid, also known as niacin, exerts its effects on lipid profile and cardiovascular risk through various mechanisms, including activation of GPR109A, inhibition of adenylyl cyclase activity, and modulation of lipid synthesis pathways. It reduces triglycerides and LDL cholesterol levels while increasing HDL cholesterol levels. Nicotinic acid also impacts apoB degradation, LDL particle formation, and CETP activity, leading to improved lipid profiles. Clinical studies have shown its benefits in reducing cardiovascular events and mortality.

Figure 1. Nicotinic Acid
Mechanism of Action
The mechanisms by which Nicotinic Acid(NA) achieves its beneficial effects remain elusive. Regarding the NA-associated reduction in triglyceride and LDL cholesterol levels, data are controversial. NA exerts its hypolipidemic effect partly through binding and activating the adipose tissue G-protein receptor-109A (GPR109A).
GPR109A activation in adipose tissue induces a Gi-mediated inhibition of adenylyl cyclase activity, thereby resulting in a decrease of cyclic adenosine monophosphate (cAMP) intracellular levels. This leads to decreased lipolysis, as cAMP is the main intracellular mediator of prolipolytic stimuli. cAMP normally activates protein kinase A to phosphorylate various proteins, including perilipin and hormone-sensitive lipase, thereby promoting lipolysis. The decrease in circulating free fatty acids results in a substrate shortage for hepatic very low-density lipoprotein (VLDL) production, consequently reducing plasma levels of LDL cholesterol and triglycerides. In addition, NA limits the hepatic triglyceride synthesis via inhibition of diacylglycerol acyl transferase 2, a key enzyme in hepatic triglyceride synthesis. Moreover, currently other mechanisms involving modulation of transcription and translation pathways are emerging. In fact, the NA-induced triglyceride synthesis inhibition has been demonstrated to create a favorable environment for protease-mediated intracellular apolipoprotein B (apoB) degradation in hepatocytes, thereby resulting in decreased apoB-containing VLDL and thus LDL particle formation. In addition, Nicotinic Acid has been demonstrated to inhibit peroxisome proliferator-activated receptor gamma (PPARg) coactivator-1beta (PGC-1b). PGC-1b is a transcriptional co-activator that normally induces hypertriglyceridemia by both stimulating hepatic lipogenesis and lipoprotein secretion and inhibiting apolipoprotein E (apoE)-driven clearance of triglyceride-rich lipoprotein via stimulating apolipoprotein C3 (apoC3) expression.1
Effect on lipid profile and cardiovascular risk
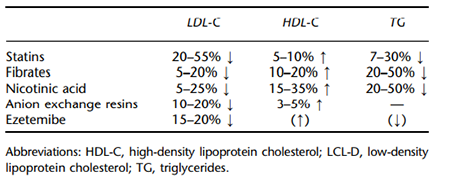
Nicotinic acid has been widely used to treat a wide range of lipid disorders and to prevent clinical atherosclerotic cardiovascular disease. It has favorable effects on all traditional measured lipid parameters and is the most potent available agent to raise high-density lipoprotein cholesterol (HDL-C). It not only increases HDL-C and apolipoprotein (apo) AI but also reduces atherogenic apoB containing low-density lipoprotein cholesterol (LDLC), very low-density lipoprotein cholesterol (VLDL-C), lipoprotein (a), and triglycerides.
Several clinical trials demonstrated that treatment with nicotinic acid, either alone or in combination with other lipidlowering agents, significantly reduced total mortality and coronary events, and retarded the progression and induced regression of atherosclerosis. Brown et al. demonstrated in the HDL Atherosclerosis Treatment Study (HATS) that the combination of niacin and simvastatin led to a statistically significant lower incidence of clinical cardiovascular events (coronary death, myocardial infarction, strokes, or revascularization for worsening ischemia) compared with placebo. In the more recent Arterial Biology for the Investigation of the Treatment Effects of Reducing Cholesterol (ARBITER 2) study, the addition of extended-release niacin (1000 mg) to ongoing statin therapy in 167 patients with known CHD and low HDL-C slowed the atherosclerotic progression of carotid intima-media thickness (CIMT) by ultrasound, relative to placebo. In a 1-year extension to this study (ARBITER 3), CIMT was reduced by 0.027 mm (P < 0.001 vs. placebo), demonstrating a regression of carotid atherosclerosis.2
References:
[1] VAIJINATH S KAMANNA M L K Anthony Vo. Nicotinic acid: recent developments.[J]. Current Opinion in Cardiology, 2008, 23 4. DOI:10.1097/HCO.0b013e3283021c82.[2] ANASTAZIA KEI M S E. Nicotinic acid: clinical considerations.[J]. Expert Opinion on Drug Safety, 2012, 11 4. DOI:10.1517/14740338.2012.682981.
You may like
Related articles And Qustion
See also


Lastest Price from Nicotinic acid manufacturers

US $0.00/kg2025-09-28
- CAS:
- 59-67-6
- Min. Order:
- 1kg
- Purity:
- 98%
- Supply Ability:
- 1000kg

US $0.00-0.00/Kg/Drum2025-04-21
- CAS:
- 59-67-6
- Min. Order:
- 1KG
- Purity:
- 99%-101%; USP
- Supply Ability:
- 1000kgs