Dehydroepiandrosterone: A Comprehensive Examination
Introduction
Dehydroepiandrosterone (DHEA) and its sulfate (DHEA-S) are the most abundant steroid hormones in the human body. Among all steroids, DHEA and DHEA-S have the highest concentrations in peripheral blood, up to 10 µM. Currently, DHEA is only used clinically to treat vaginal atrophy and dyspareunia. As an oral drug, DHEA is considered promising for the treatment of osteoporosis, cachexia, and sarcopenia, and 10% ointment can also be used for skin and muscle regeneration. In addition, DHEA's metabolite 5-androstenediol (5-AED) is a promising candidate for the treatment of acute radiation syndrome and an immunostimulant during radiopharmaceutical therapy.

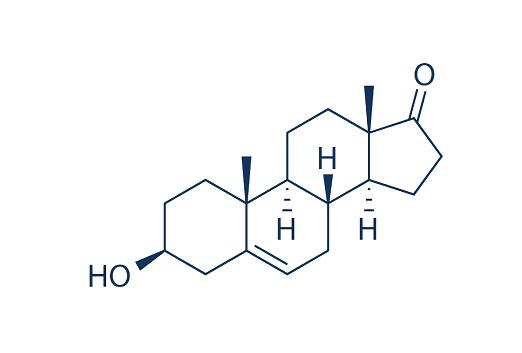
Figure 1 Characteristics of Dehydroepiandrosterone
DHEA is a precursor of the steroids androstenediol, androstenedione, testosterone (T), dihydrotestosterone (DHT), estrone, and 17β-estradiol (E2), and its biological effects may partially overlap with the androgenic and estrogenic activities of these steroids. Some studies indicate that daily long-term (for 12 months)
supplementation of 50 mg of micronized DHEA increases the circulating levels of DHEA,
DHEA-S, and androstenedione in both sexes, but testosterone levels increased to a
lower limit of normal levels only in women. Since the steroids 5-AED and DHEA
are considered immunomodulators and radioprotectors, their effect on the host immune
system is obvious. With age, the concentrations of these hormones decrease sharply, though
not as sharply as those of testosterone and estradiol, which affects the overall immune resistance of an aging person.
Biosynthesis and Transformation of DHEA
DHEA and DHEA-S are synthesised in the adrenal glands and only a small proportion (about 8-10%) is produced by the gonads. DHEA and DHEA-S are synthesised de novo in the brain and spinal cord as their concentrations in these organs are higher than in plasma and remain high after adrenalectomy and gonadectomy. DHEA is produced in the steroidogenic process mainly by two classes of steroidogenic enzymes P450s and hydroxysteroid dehydrogenases. In addition, DHEA can be sulfated to DHEA-S by steroid sulfotransferases (SULT), and the conversion of DHEA-S into DHEA is mediated by steroid sulfatase (STS) (Figure 1a). The activity and expression of hydroxysteroid dehydrogenase in the prostate determines whether the final effect is androgenic or oestrogenic. Most of the DHEA is sulfated and some of the DHEA is converted into androstenediol via AKR1C3 (Fig. 1b). The rest of DHEA and androstenediol can be converted into the corresponding ∆4 products by the hydroxysteroid dehydrogenase isoenzyme 3B2, producing 4-androstenedione (A4) and testosterone, respectively. A4 is another substrate for testosterone production by AKR1C3.
Biosynthesis of DHEA.(b)Transformation of DHEA.")
Clinical Use of DHEA
DHEA Vaginal Gel
Clinical studies have shown improvement in symptoms of vulvar and vaginal atrophy following treatment with 6.5 mg of DHEA (Intrarosa) in two 12-week placebo-controlled efficacy trials. It also reduced symptoms of vaginal severity in patients with breast and gynaecological cancers.
In addition, clinical trials confirmed the effectiveness of DHEA at a daily intravaginal administration of 0.50% (6.5 mg) for vulvovaginal atrophy and dyspareunia. Moreover, the effect
of DHEA does not extend to the endometrium; it works only in the vagina, and serum
sex steroids remain within the biologically low postmenopausal reference range, which
rules out any stimulation of the already atrophic endometrium.
Anti-aging effect
The regenerative effects of DHEA on fibroblasts from different tissues have been reported. DHEA not only stimulates the proliferation and viability of fibroblasts, but also upregulates the levels of skin regeneration proteins in cultured human skin fibroblasts. It increases collagen production in a dose-dependent manner, with the effect being maximal at 10 µM. It also increases the levels of alpha1 procollagen mRNA by 1.6-fold and decreases the expression of collagen metabolic enzymes. This suggests that topical skin application of DHEA has modest benefits. In addition, there are studies that suggest that taking DHEA supplements may improve skin hydration and firmness and reduce age spots in the elderly.
Osteoporosis
Numerous clinical and animal studies have demonstrated the promise of DHEA in the treatment of osteoporosis. One of the main causes of osteoporosis is a decline in sex hormone levels. Clinical studies have shown that BMD increases after DHEA treatment, which is due to DHEA's ability to increase osteoblast activity and the expression of insulin-like growth factor 1 (IGF-1). The osteogenic effects in the elderly are consistent with the estrogenic and androgenic activities of DHEA, which is a precursor of active androgens and estrogens in local tissues such as bone. Therefore, it stimulates osteoblastogenesis. DHEA replacement may also increase levels of IGF-1, which may contribute to its anabolic effects.
References:
[1] KRZYSZTOF RUTKOWSKI. Dehydroepiandrosterone (DHEA): hypes and hopes.[J]. Drugs, 2014, 74 11. DOI:10.1007/s40265-014-0259-8.[2] P H WILLEMSE B G W L D Dikkeschei. Physiological importance of dehydroepiandrosterone.[J]. The Lancet, 1994, 344 8920.
[3] TATIANA A FEDOTCHEVA. Dehydroepiandrosterone and Its Metabolite 5-Androstenediol: New Therapeutic Targets and Possibilities for Clinical Application.[J]. Pharmaceuticals, 2024, 17 9. DOI:10.3390/ph17091186.
You may like
Related articles And Qustion



Lastest Price from Dehydroepiandrosterone manufacturers

US $600.00/kg2025-11-24
- CAS:
- 53-43-0
- Min. Order:
- 1kg
- Purity:
- 99
- Supply Ability:
- 999

US $5.00-0.50/KG2025-05-07
- CAS:
- 53-43-0
- Min. Order:
- 1KG
- Purity:
- 99% hplc
- Supply Ability:
- 500TONS