Antimicrobial Activity and Susceptibility of Ampicillin and ampicillin-like agents
Ampicillin and ampicillin-like agents, such as amoxicillin, have many similar properties, but also some important differences. They are all semisynthetic penicillins derived from the penicillin nucleus, but differ in their bioavailability and pharmacokinetic features. The two key agents in this group are ampicillin and amoxicillin, in terms of both their individual properties and the fact that they have both been combined with the beta-lactamase inhibitors, sulbactam and clavulanic acid (Amoxicillin–Clavulanic Acid (Co-Amoxiclav)), respectively, to broaden their antibacterial spectrum of activity. These individual agents will be discussed in this chapter.
1a. Ampicillin
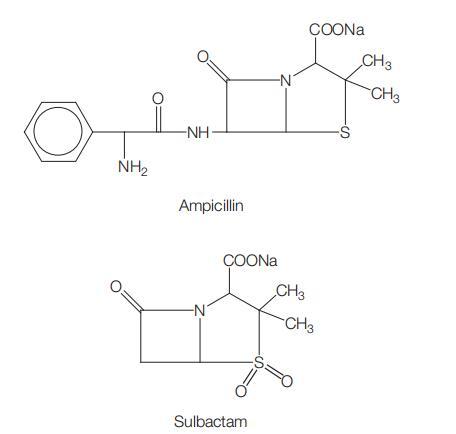
Ampicillin (AMP) is a semisynthetic penicillin derived from the penicillin nucleus, 6-APA (see Chapter 1, Benzylpenicillin (Penicillin G)). It has been replaced in most countries by amoxicillin, which is better absorbed from the intestinal tract. The chemical structure of ampicillin is shown in Figure 3.1.
1b. Ampicillin-like penicillins
Ampicillin has been modified chemically in various ways in an attempt to produce improved compounds; eight such modifications have been available. Amoxicillin, epicillin, and cyclacillin have intrinsic antibacterial activity, but the other five antibiotics (esters, prodrugs) are hydrolyzed in the body to ampicillin after administration. Most of these compounds exhibit no, or only marginal, superiority over ampicillin (Dyas and Wise, 1983). Amoxicillin has significant advantages over ampicillin and has largely replaced it, at least for oral administration. The chemical structures of amoxicillin and other ampicillin-like compounds are shown in Figure 3.1.

Amoxicillin: Chemically, amoxicillin (AMOX) is alpha-amino-phydroxybenzyl- penicillin. Developed by Beecham Research Laboratories (Sutherland et al., 1972), its main advantage over ampicillin is its better absorption from the gastrointestinal tract. It is available as amoxicillin trihydrate for oral administration and sodium amoxicillin, for parenteral use. In many regions, it has replaced ampicillin in common clinical practice.
Epicillin: Chemically, this is 6-[D2-amino-2-(1,4-cyclohexadienyl)
acetamido]-penicillanic acid (Basch et al., 1971).
Cyclacillin: This is a partially penicillinase-resistant penicillin with a
chemical formula 6-(1-aminocyclo-hexanecarboxamide)-penicillanic
acid (Gonzaga et al., 1974).
Hetacillin: Developed by Bristol Laboratories in 1965 by reacting ampicillin with acetone, this is also referred to as phenazacillin. Hetacillin hydrolyzes in solution to form ampicillin both in vitro and in vivo, therefore its ultimate active component is mainly ampicillin (Sutherland and Robinson, 1967; Kahrimanis and Pierpaoli, 1971). Pivampicillin: This is the hydrochloride salt of pivaloyl-oxymethyl-Dalpha- aminobenzyl-penicillinate, which is an ampicillin ester. It is better absorbed from the gastrointestinal tract than ampicillin, to which after absorption it is rapidly and completely hydrolyzed in the tissues and blood (Von Daehne et al., 1971).
Talampicillin: This is a thiazolide carboxylic ester of ampicillin. It has no antibacterial activity until it is hydrolyzed by tissue esterases in the intestinal wall to form ampicillin, which is then rapidly absorbed. Serum levels after administration of this drug are approximately twice those attained with an equivalent dose of ampicillin (Clayton et al., 1974; Leigh et al., 1976).
Bacampicillin: This is another ester of ampicillin which is chemically 1u-ethoxycarbonyloxy-ethyl 6-(D-alpha-aminophenylacetamido) penicillinate. After absorption, it is rapidly hydrolyzed to ampicillin by esterases present in the serum and in the intestinal wall. Serum levels achieved are two to three times higher than those after equivalent doses of ampicillin (Bodin et al., 1975; Neu, 1981). Metampicillin: This is produced by combining ampicillin with formaldehyde. When administered orally, it is rapidly hydrolyzed to ampicillin in the gut, and administered in this way it has no advantages over ampicillin. After parenteral administration, some of the drug apparently circulates as unchanged metampicillin, because it has a greater stability in serum than in aqueous acid solutions. It is excreted into the bile in a greater concentration than ampicillin (Neu, 1975).
The last seven compounds have no special advantages over amoxicillin and in recent years they have been used very little, if at all, in most countries. They will therefore not be described any further in this chapter.
ANTIMICROBIAL ACTIVITY
The in vitro activities of ampicillin and, amoxicillin (AMP–AMOX) are very similar and, unless notable differences occur, are discussed together. The European Committee on Antimicrobial Susceptibility Testing (EUCAST) wild-type and clinical breakpoints for AMP and AMOX among common bacterial pathogens are shown in Table 3.1.

Figure 3.1 Chemical structure of ampicillin and other ampicillin-like drugs: (a) ampicillin, (b) amoxicillin, (c) epicillin, (d) cyclacillin, (e) hetacillin, (f) pivampicillin, (g) talampicillin, (h) bacampicillin, and (i) metampicillin.
2a. Routine susceptibility
In vitro, amoxicillin is virtually the same as ampicillin, although it has its own intrinsic activity and it is not converted to ampicillin in the body (Sutherland et al., 1972; Cole and Ridley, 1978). There are only a few differences between the antibacterial actions of these drugs. Amoxicillin is about 2-fold more active than ampicillin against Enterococcus faecalis and Salmonella spp., but 2-fold less active against Shigella spp. (Sabto et al., 1973; Neu, 1974). Haemophilus influenzae also appears to be slightly less sensitive to amoxicillin than to ampicillin (Kosmidis et al., 1972); the same is true for Gram-positive and Gram-negative anaerobic bacteria (Sutter and Finegold, 1976). These drugs are active against most of the bacteria sensitive to penicillin G, but, in addition, also against some Gram-negative bacilli which are penicillin G resistant.
Gram-positive cocci
AMP–AMOX are essentially as active against many of these as penicillin, including Streptococcus pyogenes, S. pneumoniae, and S. viridans. Pneumococcal strains which are relatively resistant to penicillin G are also usually relatively resistant to AMP–AMOX to the same degree (see Chapter 1, Benzylpenicillin (Penicillin G)) (Jorgensen et al., 1990; Powell et al., 1991). Pneumococcal strains that are completely penicillin G resistant are also invariably completely amoxicillin resistant. While amoxicillin generally retains more clinically useful activity than penicillin or ampicillin against pneumococci because of its improved pharmacokinetics, this is by no mean always the case (du Plessis et al., 2002).
Gram-positive bacilli
Corynebacterium diphtheriae and Bacillus anthracis are usually sensitive to AMP–AMOX. Listeria monocytogenes is also usually sensitive to a degree similar to that to penicillin G. Whether these drugs are bactericidal to L. monocytogenes depends on the conditions under which the test is performed; after normal subculture after a 24-hour incubation, MICs of ampicillin are low (0.24 mg/ml), but MBCs are high (15.6–125.0 mg/ml) (Penn et al., 1982); if subcultures are performed after a 48-hour incubation, ampicillin is bactericidal to most strains in low concentrations (Winslow et al., 1983).
Gram-negative bacilli
In contrast to penicillin G, AMP–AMOX are active against some of these bacteria (Rolinson and Stevens, 1961). Escherichia coli may be sensitive, but many strains are resistant. This is particularly so in hospitals, where more than 50% of E. coli strains can be ampicillin resistant (Yoshioka et al., 1977; Cooksey et al., 1990; Gransden et al., 1990; Spencer et al., 1990; Burman et al., 1992). Ampicillin-resistant E. coli strains also occur in community-acquired infections (Sogaard, 1975; Levy et al., 1988; Chamberland et al., 1992).
Gram-negative anaerobic bacteria
Some strains, e.g. of Bacteroides melaninogenicus and the Fusobacterium spp., may be AMP–AMOX sensitive unless they produce betalactamase, but B. fragilis is resistant. Other Bacteroides spp. vary in sensitivity, but less than 50% of isolates are inhibited by low AMP– AMOX concentrations (Sutter and Fbinegold, 1976; Stark et al., 1993).
Other organisms
The leptospirae are AMP–AMOX sensitive (Oie et al., 1983). Mycoplasmas and Rickettsiae are resistant. Mycobacteria spp. are also resistant.
2b. Emerging resistance and cross-resistance
Resistance to AMP–AMOX has emerged substantially in many common human pathogens in the past few decades.
Enterococci
In the 2006 EARSS report (see Table 3.2), in which 29 European countries reported on 6510 invasive isolates of E. faecalis, AMP-AMOX resistance was at fairly low levels in E. faecalis (EARSS, 2006). However, only Iceland (3%), France (16%), Sweden (20%), and Romania (15%) reported aminoglycoside resistance <25%, the majority of countries reporting high-level aminoglycoside resistance in 25–50% of invasive isolates of E. faecalis.

Salmonella spp.
Salmonella spp. are increasingly resistant to AMP–AMOX. Antibiotic resistance to multiple agents in salmonellae is usually mediated by plasmids. By comparing the molecular structure of plasmids derived from multiresistant salmonella strains of human and animal origin, O’Brien et al. (1982) showed that such strains were spread from animals to humans in the USA, as observed in the UK. This was confirmed in the USA when antimicrobial-resistant Salmonella newport of animal origin caused serious human disease (Holmberg et al., 1984). In the USA, ampicillin-resistant S. typhimurium increased in frequency from 1970, reaching about 40% by 1975, when about 10% of other Salmonella spp. had also become ampicillin resistant. Associated resistance to streptomycin, tetracyclines, and sulfonamides was quite common, but chloramphenicol resistance was rare.
Shigella spp.
Resistance among strains of Shigella spp. is increasing substantially. Originally infrequent, ampicillin-resistant Shigella strains (mainly S. sonnei) rose to over 80% in some areas of the USA (Ross et al., 1972; Tilton et al., 1972). During the 1970s, ampicillin-resistant shigellae became prevalent in many cities of the USA. Neu et al. (1975b) investigated ampicillin sensitivity of 102 S. sonnei and 14 S. flexneri strains isolated from patients in the New York City hospital; S. flexneri strains were sensitive, but resistance was present in 60% of S. sonnei strains. Of isolates from patients in Houston, Texas, 55% of S. sonnei (113 strains) and 7% of S. flexneri (56 strains) were ampicillin resistant (Byers et al., 1976). These shigellae were also usually resistant to sulfonamides, streptomycin, and tetracyclines. This multiple resistance was R plasmid mediated (Prince and Neu, 1976).
Helicobacter pylori
Resistance to AMP–AMOX among H. pylori strains is increasing (see Table 3.3), as is resistance to other agents (see Chapter 90, Metronidazole). Amoxicillin resistance, which is associated with failure of eradication (Dore et al., 1998), has been shown to be due to modified PBP1A (Paul et al., 2001; Okamoto et al., 2002). Interniche heteroresistance has been described (Matteo et al., 2008), which might easily be missed, particularly if multiple biopsies are not taken. Multiple amino acid substitutions in the transpeptidase region of PBP- 1 have now been described in association with different MICs (Rimbara et al., 2007). Tolerance has also been described (Dore et al., 2001).

Haemophilus influenzae
AMP–AMOX resistance among H. influenzae isolates has been detected in many countries (Bell and Smith, 1975; Bio¨rklund et al., 1975; Fallon, 1976; Jacobson et al., 1976). Ampicillin-resistant H. influenzae type b strains were isolated from children with septicemia, meningitis, epiglottitis, otitis media, and other severe childhood infections. There were also healthy nasopharyngeal carriers of the organism. Sometimes ampicillin-resistant strains have emerged in vivo during ampicillin treatment of a severe infection such as meningitis, and have been associated with recrudescence of the infection (Albritton et al., 1977; Granoff et al., 1978).
Related articles And Qustion


Lastest Price from Ampicillin manufacturers

US $10.00/kg2025-04-21
- CAS:
- 69-53-4
- Min. Order:
- 1kg
- Purity:
- 99%
- Supply Ability:
- 100 mt

US $90.00/kg2025-04-21
- CAS:
- 69-53-4
- Min. Order:
- 1kg
- Purity:
- 99% Purity (What/sapp: +86 18145728414)
- Supply Ability:
- 1000 Tons/Month