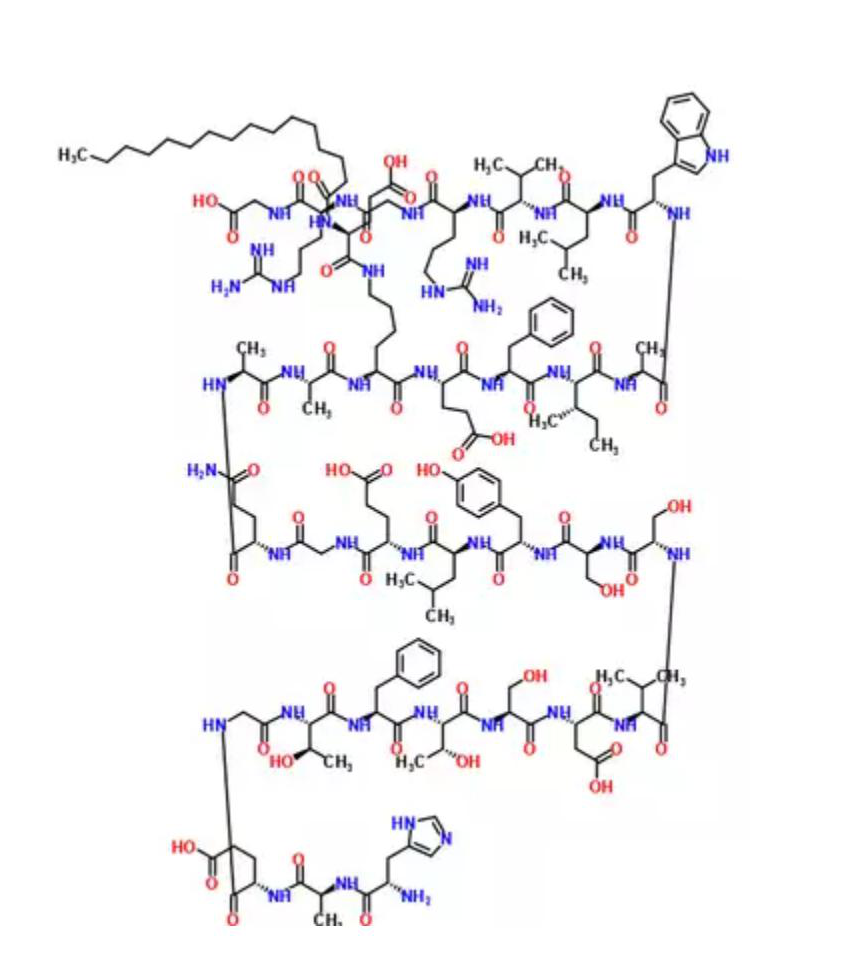
利拉鲁肽
Liraglutide
204656-20-2
204656-20-2
询价
5kg
起订
10kg
起订
浙江 更新日期:2021-03-26
产品详情:
公司简介
一般项目:第二类医疗器械销售;针纺织品及原料批发;服装复试批发;日用百货销售;家用电器销售;第一类医疗器械销售;化工产品销售(不含许可类化工产品);五金产品批发;计算机软硬件及辅助设备批发;化妆品批发;消毒剂销售(不含危险化学品);专用化学产品销售(不含危验化学品);个人卫生用品销售;金属材料售;医用口罩批发;日用口罩(非医用)销售;医护人员防护用品批发;卫生用品和一次性使用医疗用品销售;劳动保护用品确售;合成材料销售;饲料添加剂销售;药物检测仪器销售;制药专用设备销售;财务咨询;信息咨询服务(不含许可类信息咨询服务);技术服务、技术开发、技术咨询、技术交流、技术转让、技术推广;染料销售;卫生用品销售;建筑装饰材料销售;电子办公设备销售;针纺识品销售;贸易经纪;销售代理;国内贸易代理(除依法须经批准的项目外,凭营业执照依法自主开展经营活动)。许可项目∶食品经营(销售预包装食品);货物进出口;药品进出口;进出口代理;技术进出口(依法须经批准的项目,经相关部门批批准方可开展经营活动,具体经营项目以审批结果为准)。
| 成立日期 | (23年) |
| 注册资本 | 1000万人民币 |
| 员工人数 | 1-10人 |
| 年营业额 | ¥ 100万以内 |
| 经营模式 | 贸易 |
| 主营行业 | 中间体,医药原料 |
利拉鲁肽相关厂家报价 更多
-
- 利拉鲁肽
- 杭州信海医药科技有限公司 VIP
- 2026-06-19
- ¥6000
-
- 利拉鲁肽/204656-20-2/Liraglutide/多肽
- 南京肽研生物科技有限公司 VIP
- 2026-06-19
- ¥400
-

- 利拉鲁肽;204656-20-2
- 湖北摩科生物科技有限公司 VIP
- 2026-06-18
- 询价
-

- 利拉鲁肽 liraglutide 204656-20-2
- 成都彼样生物科技有限公司 VIP
- 2026-06-18
- 询价
-

- 利拉鲁肽
- 苏州默迪夫生物科技有限公司 VIP
- 2026-06-18
- 询价
-

- 利拉鲁肽
- 常州市宣明医药科技有限公司 VIP
- 2026-06-18
- ¥4000
-

- 利拉鲁肽;99.8%利拉鲁肽原粉;204656-20-2
- 湖北鸿运隆生物科技有限公司 VIP
- 2026-06-18
- 询价
-
- 利拉鲁肽,Liraglutide
- 成都圣诺生物制药有限公司
- 2026-06-18
- 询价
-

- Liraglutide
- 合肥赛曼诺生物科技有限公司 VIP
- 2026-06-18
- 询价
-
- 利拉鲁肽 204656-20-2
- 湖北丽都新材料科技有限公司 VIP
- 2026-06-17
- 询价
