To a slurry of 110.5 g of 14-hydroxydihydronormorphinone in 2.5 liters of
methylene chloride and 280 ml of triethylamine was added a solution of 106 g
of cyclobutanecarboxylic acid chloride in 500 ml of methylene chloride. The
temperature of the reaction mixture was maintained at 20°C to 25°C during
the addition. After 5 minutes the reaction mixture was brought to reflux and
heated for 5 hours.
It was then cooled, washed with water, dried over sodium sulfate and
evaporated to dryness. The residue was crystallized from benzene and
pentane to give 138.5 g of the dicyclobutanecarbonyl derivative, melting point
about 112°C (dec.).
The dicyclobutanecarbonyl derivative (136.7 g) was dissolved in 200 ml of
tetrahydrofuran and added dropwise to a suspension of 34.2 g of lithium
aluminum hydride in 1 liters of tetrahydrofuran. The temperature of the
mixture rose to reflux during the addition. Reflux was maintained for 2 hours
after the addition was completed. After cooling, 110 ml of ethyl acetate was
added dropwise, followed by 30 ml of water, followed by a solution of 53 g of
ammonium chloride in 125 ml of water. The resulting mixture was filtered and
the inorganic precipitate was washed with methanol. Evaporation of the
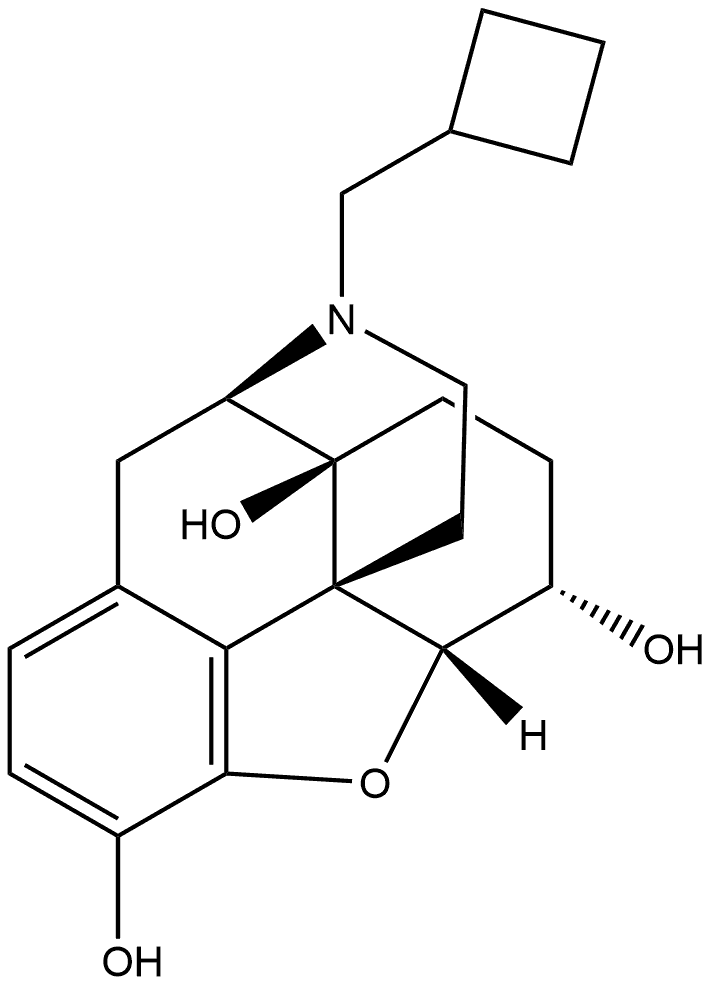
combined filtrates gave 66 g of N-cyclobutylmethyl-14-hydroxydihydronormorphinone, melting point 229°C to 231°C.
Nalbuphine (Nubain) is a mixed agonist–antagonist that
is similar in structure to both the antagonist naloxone
and the agonist oxymorphone. It is administered parenterally
and is equipotent to morphine and 5 times as
potent as pentazocine.Although the pharmacological effects
(analgesia, respiratory depression, sedation, and so
on) are similar to those produced by pentazocine, nalbuphine
produces fewer psychotomimetic effects. It differs
from pentazocine in that it has far greater antagonist
than agonist effect.Thus, its use is likely to precipitate severe
withdrawal in opioid-dependent patients. It is used
much as pentazocine is, that is, for moderate to severe
pain, postsurgical anesthesia, and obstetrical analgesia.
Nalbuphine’s abuse potential is less than that of codeine
and propoxyphene, although tolerance and dependence
have been shown following chronic administration. High
doses are perceived by addicts as being like those of the
barbiturates.Drug interactions and contraindications are
similar to those for pentazocine and morphine.
Nalbuphine (Nubain) is structurally a member of thephenanthrene class of compounds and resembles oxymorphonewith a cyclobutyl methyl group on the nitrogen,equivalent to naloxone’s substitution. It was introduced in1979 as an agonist/antagonist with the hope of becoming aneffective pain reliever with little abuse potential. Althoughthe abuse potential of nalbuphine is low, it is not zero, andincreasing reports of diversion and abuse can be found in theliterature and the Internet. At low parenteral doses(<0.5 mg), it has an analgesic potency approximately twothirds that of morphine, and it has a similar degree of respiratorydepression. However, escalating doses above 30 mgdoes not produce further respiratory depression. The oralbioavailability of nalbuphine is only 12%, and the drug isonly marketed as an injectable. Patents have been filed foran oral extended-release formulation, and it is presently inphase II testing. The pharmacologic profile of nalbuphinein animal studies includes agonist activity at the κ-receptorand antagonist activity at the μ-receptor. Clinical studieshave shown that nalbuphine, and κ-agonists in general, mayhave better analgesic activity in female patients comparedwith male patients. Used as the sole opioid agent, nalbuphinehas been used successfully to treat the pain of labor,cesarean section, dental extraction, hip replacement, andhysterectomy surgery. Nalbuphine also may have a role intreating opioid-induced pruritus, because it can reverse thepruritus without reversing the analgesic effect when used inlow doses. Nalbuphine is marketed as an injectable (10 and20 mg/mL).