Omeprazole: Mechanism of Action, Pharmacokinetics and Pharmacodynamics
General Description
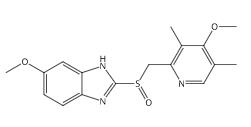
Omeprazole is a potent proton pump inhibitor that reduces gastric acid secretion by covalently binding to the H+/K+-ATPase enzyme in gastric parietal cells. It is activated in the acidic environment of the stomach and inhibits acid secretion effectively for over 24 hours despite its short plasma half-life of approximately 60 minutes. Omeprazole's pharmacokinetics are influenced by its formulation, with about 50% oral bioavailability. It is primarily metabolized in the liver, and its effects on gastric acid secretion vary among individuals. Long-term use does not significantly impair vitamin B12 levels, but monitoring is essential for prolonged treatment.

Figure 1. Omeprazole
Mechanism of Action
Mechanism in Acid Secretion
Omeprazole is a powerful medication designed to inhibit gastric acid secretion by targeting the H+/K+-ATPase enzyme. This enzyme, also known as the proton pump, is crucial in the production of hydrochloric acid in the stomach. It operates by exchanging hydrogen ions for potassium ions across the membrane of gastric parietal cells. In its inactive state, the H+/K+-ATPase is located within vesicles in the cell cytoplasm. When the parietal cells are stimulated, such as by histamine, the enzyme moves to the plasma membrane where it becomes active. Omeprazole interferes with this process by directly inhibiting the proton pump's ability to secrete acid. 1
Active Form and Inhibition
Omeprazole is a lipophilic weak base that becomes protonated in the acidic environment of the stomach's secretory canaliculus. This transformation traps omeprazole inside the parietal cells, where it is converted into its active form, a sulfename. This active form then binds covalently to the cysteine residues on the H+/K+-ATPase enzyme, effectively blocking its function. This inhibition reduces acid secretion, leading to a decrease in stomach acidity. The effects of omeprazole persist until new H+/K+-ATPase proteins are synthesized, given the enzyme's half-life of approximately 18 hours. 1
Pharmacokinetics and Pharmacodynamics
Pharmacokinetics
Omeprazole is a proton pump inhibitor that exhibits unique pharmacokinetic properties due to its susceptibility to gastric acid degradation. This characteristic significantly impacts its oral bioavailability, which is approximately 50 percent when formulated in pH-sensitive granules. These granules dissolve and release omeprazole only when the pH in the gastrointestinal tract exceeds 6, promoting improved absorption. Following oral administration of omeprazole, peak plasma concentrations are observed within two to four hours. It is noteworthy that the plasma half-life of omeprazole is around 60 minutes; however, its duration of action extends beyond 24 hours. This extended effect results from omeprazole's covalent binding to H+/K+-ATPase in the gastric parietal cells, establishing a longer-lasting inhibition of gastric acid secretion. The relationship between omeprazole plasma concentration and acid inhibition is indirect, as the inhibition is more closely related to the area under the plasma concentration-time curve rather than the immediate plasma levels. 2
Pharmacodynamics
The pharmacodynamics of omeprazole are characterized by its ability to inhibit gastric acid secretion effectively. A single 20-mg dose of omeprazole can reduce acid secretion by approximately 65 percent within 4 to 6 hours post-administration and maintains a reduction of about 25 percent after 24 hours. Upon administration of multiple doses, the inhibition of acid secretion increases due to enhanced bioavailability and the saturation of more H+/K+-ATPase molecules. Interestingly, the degree of acid secretion inhibition varies among individuals, with steady-state inhibition ranging from 35 to 65 percent. This variability diminishes with increased doses of omeprazole, where higher doses lead to more profound and consistent acid secretion inhibition. Moreover, upon cessation of treatment, it can take up to three days for gastric acid secretion to return to baseline levels, but rebound hypersecretion does not occur, illustrating the stable inhibition capacity of omeprazole. 1, 2
Metabolism and Other Effects
Omeprazole undergoes extensive metabolism primarily in the liver, with its major metabolites being sulfone derivatives and hydroxyomeprazole, neither of which inhibits gastric acid secretion. Approximately 80 percent of oumeprozole metabolites are excreted in urine, while the remainder is eliminated via feces after biliary excretion. Importantly, the pharmacokinetics of omeprazole are generally unchanged in patients with renal impairment; however, older adults and individuals with liver dysfunction exhibit slower metabolism and increased bioavailability. Despite these variations, no dosage adjustments are typically necessary in these populations. While omeprazole does not significantly affect intrinsic factor secretion and vitamin B12 absorption from protein sources, it may reduce the absorption of bound vitamin B12. The long-term usage of omeprazole does not significantly impair vitamin B12 levels, and its effects on gastrointestinal hormones, such as gastrin, may indirectly relate to the risk of gastric carcinoid tumors observed in animal studies. Comprehensive understanding of the pharmacodynamics and pharmacokinetics of omeprazole underscores its therapeutic efficacy and the need for monitoring in long-term use. 1, 2
References:
[1] C CEDERBERG I S T Andersson. Omeprazole: pharmacokinetics and metabolism in man.[J]. Scandinavian journal of gastroenterology. Supplement, 1989, 166. DOI:10.3109/00365528909091241.
You may like
Related articles And Qustion

Lastest Price from Omeprazole manufacturers

US $0.00/kg2025-09-28
- CAS:
- 73590-58-6
- Min. Order:
- 1kg
- Purity:
- 98%
- Supply Ability:
- 1000kg

US $5.00-0.50/KG2025-05-07
- CAS:
- 73590-58-6
- Min. Order:
- 1KG
- Purity:
- 99% hplc
- Supply Ability:
- 500TONS