Doripenem: Antimicrobial Activity, Susceptibility, Administration and Dosage, Clinical Uses etc.
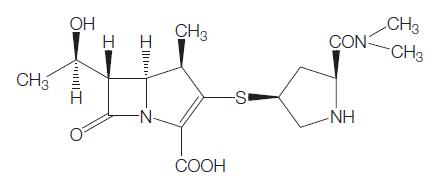
The chemical structure of doripenem is similar to that of meropenem (Anderson, 2006) (see Figure 38.1). In doripenem, the dimethylycarbamoyl side chain of meropenem is replaced by a sulfamoylaminomethyl group (Jones et al., 2004b; Anderson, 2006).
The antibacterial spectrum of doripenem is very similar to meropenem. Doripenem is active against a broad range of Grampositive and Gram-negative bacteria, including both aerobes and anaerobes, but Mycoplasma spp., Chlamydia spp., Legionella spp., Stenotrophomonas maltophilia, Burkholderia cepacia, Clostridium difficile, methicillin-resistant Staphylococcus aureus (MRSA), and Enterococcus faecium are not within its antimicrobial spectrum.
Doripenem is the latest addition to carbapenem-class antibiotics. Doripenem was launched in 2005 in Japan under the Japanese trade name, Finibaxs. The rights to the drug outside Japan were subsequently acquired by Peninsula Pharmaceuticals Inc., and then Johnson & Johnson. Doripenem was approved by the US Food and Drug Administration (FDA) in October 2007 for complicated intra-abdominal infection and complicated urinary tract infection (US trade name, Doribaxs).

Figure 38.1 Chemical structure of doripenem.
ANTIMICROBIAL ACTIVITY
a. Routine susceptibility
The in vitro activity of doripenem is summarized in Tables 38.1, 38.2, and 38.3.
Gram-positive cocci
Doripenem has potent activity against many of the common Grampositive human pathogens, as does imipenem and meropenem (see Table 38.1). Methicillin-susceptible S. aureus (MSSA) and methicillinsusceptible coagulase-negative staphylococci are doripenem sensitive. However, MRSA and methicillin-resistant coagulase-negative staphylococci are doripenem resistant.
Gram-positive bacilli
In vitro activity of doripenem against Bacillus spp., Listeria monocytogenes, Nocardia spp., and Rhodococcus spp. has not yet been investigated.
Many Corynebacterium spp. (e.g. C. striatum, C. accolans, C. simulans, and C. xerosis) are highly sensitive to doripenem (MIC range, r0.015–0.25 mg/ml, 18 isolates). However, some other Corynebacterium spp. (e.g. C. aurimucosum, C. jeikeium, C. minutissimum, and C. urealyticum) are relatively resistant to doripenem (MIC range, r0.25–32 mg/ml, 14 isolates) (Goldstein et al., 2008).
Gram-positive anaerobes
Clostridium perfringens and Propionibacterium spp. are nearly always doripenem sensitive. The sensitivities of Peptostreptococcus spp. are variable. The MICs of doripenem against C. difficile are between 1 and 4 mg/ml (Hecht et al., 2007; Kim et al., 2008; Snydman et al., 2008; Tanaka et al., 2009). Although doripenem seems to be effective against C. difficile in terms of its MIC, clinical efficacy for C. difficile-associated disease is unlikely. Table 38.3 summarizes the in vitro activity of doripenem against common anaerobes.
Gram-negative cocci
Moraxella catarrhalis is highly sensitive to doripenem (Fritsche et al., 2005). The sensitivity of Neisseria spp. to doripenem has not been investigated.

Table 38.1 In vitro susceptibility of selected Gram-positive organisms to doripenem.
Gram-negative bacilli
Haemophilus influenzae, including beta-lactamase-producing strains, are doripenem sensitive (Fritsche et al., 2005). Other Haemophilus spp. are also doripenem sensitive (MIC90, 0.5 mg/ml) (Brown and Traczewski, 2005).
Aeromonas spp. are generally sensitive to doripenem (MIC90, 1mg/ ml), although strains with an MIC of 4 mg/ml have been recovered (Fritsche et al., 2005).
The sensitivities of Campylobacter spp., Helicobacter pylori, Pasteurella multocida, and other uncommon Gram-negative bacilli to doripenem have not been investigated.
Gram-negative anaerobes
Doripenem has reliable in vitro activity against anaerobic clinical isolates, including the Bacteroides fragilis group, Prevotella spp., Porphyromonas spp., and Fusobacterium spp. (Wexler et al., 2005; Hecht et al., 2007; Credito et al., 2008; Goldstein et al., 2008). Fewer than 10% of B. fragilis strains have doripenem MICs greater than 1 mg/ ml (Wexler et al., 2005; Credito et al., 2008), but a very occasional strain has had MICs as high as 16 mg/ml (Wexler et al., 2005). Sutterella wadsworthensis is generally resistant to doripenem (MIC50, 4mg/ml) (Wexler et al., 2005).

 In vitro susceptibility of selected Gram-negative organisms to doripenem.
In vitro susceptibility of selected Gram-negative organisms to doripenem.
b. Emerging resistance and cross-resistance
The issue of emerging resistance to doripenem is quite similar to that for imipenem and meropenem. Emerging resistance of Gram-negative bacilli to carbapenems has been problematic worldwide and doripenem cannot overcome most of the prevalent carbapenem resistance mechanisms. In Gram-negative bacilli, the most important mechanism of resistance is production of beta-lactamases capable of significant carbapenem hydrolysis (Mushtaq et al., 2004a; Mushtaq et al., 2004b). The most prominent examples are the KPC beta-lactamases, metallobeta- lactamases (for example, IMP or VIM types), and some OXA type beta-lactamases produced by Acinetobacter baumannii (Mushtaq et al., 2004a; Mushtaq et al., 2004b).
MECHANISM OF DRUG ACTION
A number of enzymatic activities are involved in the biosynthesis of the peptidoglycan sacculus, including cross-linking via peptide bridges by transpeptidase enzymes (Stratton, 2005). Doripenem, like other beta-lactam antibiotics, reacts chemically with the transpeptidases (also known as penicillin-binding protein, PBPs) to form stable acylenzymes. This inactivates the PBPs and prevents further cross-linking.
This leads to a weakened cell wall, which eventually ruptures because
of osmotic pressure forces (Stratton, 2005).
Doripenem has high affinity for PBP2 and PBP3 in P. aeruginosa and
PBP2 in E. coli (Davies et al., 2008). In general, PBP-binding profiles of doripenem are quite similar to those of meropenem. In contrast,
imipenem has greater affinity to PBP1a and PBP1b in P. aeruginosa, but
lesser affinity to PBP2 and PBP3 (Davies et al., 2008). PBP-binding
studies of wild-type penicillin-susceptible S. pneumoniae isolates show
that doripenem has good affinity for all PBPs, including PBP1a and
PBP2b (Davies et al., 2008). However, reduced affinity, particularly to
PBP2x and PBP2b, occurred in a penicillin-resistant isolate (Davies et
al., 2008).
 Table 38.3 In vitro susceptibility of selected anerobes to doripenem.
Table 38.3 In vitro susceptibility of selected anerobes to doripenem.
MODE OF DRUG ADMINISTRATION AND DOSAGE
a. Adults
Based on the current FDA-approved indications (complicated intra-abdominal infection and complicated urinary tract infection), the recommended dose for doripenem is 500 mg every 8 hours (administered over a 1-hour infusion), in patients with creatinine clearance >50 ml/min (Johnson & Johnson, 2007).
b. Newborn infants and children
Safety and effectiveness of doripenem in premature neonates, newborn infants, and children has not been established (Shionogi, 2008; Johnson & Johnson, 2009).

Table 38.4 Pharmacokinetic parameters of doripenem.
TOXICITY
The incidence and types of all adverse events in the clinical studies, and those considered drug related by the investigators, were similar in doripenem and comparator arms in all studies. The most common adverse effects were headache, nausea, diarrhea, rash, and phlebitis (Johnson & Johnson, 2007).
a. Seizures
b In animal studies performed by Shionogi & Co, doripenem lacked convulsive activity and demonstrated weak affinity for the GABA receptor compared with other beta-lactam antibiotics in in vitro binding studies (Horiuchi et al., 2006). In the open-label study comparing doripenem with imipenem for ventilator-associated pneumonia, seizures were reported in 3/262 (1.1%) patients in the doripenem arm and 10/263 (3.8%) patients in the imipenem arm (Chastre et al., 2008). In all doripenem-treated patients and in all but one of the imipenem-treated patients, seizures did not appear to be related to study drug therapy (Chastre et al., 2008).
b. C. difficile-associated diarrhea
There is minimal published information on C. difficile-associated diarrhea following doripenem usage, although it has been reported in postmarketing surveillance (Greer, 2008).
c. Hypersensitivity reactions
Cases of anaphylaxis, Stevens–Johnson syndrome, and toxic epidermal necrolysis with doripenem have been noted in postmarketing reports (Greer, 2008). It is recommended that if a patient has a history of anaphylaxis when receiving penicillins, cephalosporins, or other carbapenems, the patient should not receive doripenem (Johnson & Johnson, 2007).
CLINICAL USES OF THE DRUG
Doripenem is currently approved by the US FDA for use in patients with complicated intra-abdominal infection and complicated urinary tract infection – for which the recommended dose is 500 mg every 8 hours (administered over a 1-hour infusion; normal creatinine clearance) (Johnson & Johnson, 2007).
a. Complicated intra-abdominal infection
Lucasti et al. (2008) conducted a multicenter double-blind randomized study of doripenem (500 mg every 8 hours, over 1 hour) versus meropenem (1 g every 8 hours, over 3–5 minutes) for hospitalized adults with complicated intra-abdominal infections. A total of 476 patients were enrolled. After a minimum of nine intravenous (i.v.) doses and if adequate clinical improvement had occurred, patients could be switched to oral amoxicillin–clavulanate. In total, 68% patients received i.v. study drug followed by oral amoxicillin– clavulanate, whereas 32% received only an i.v. carbapenem. By definition, complicated intra-abdominal infections extend beyond the site of origin into the peritoneal space, causing peritonitis or abscess formation (Solomkin et al., 2003). The most common sites of infection among enrolled patients were the appendix (59.9%) and the colon (20.1%). All patients underwent surgical intervention within 24 hours of study entry (Lucasti et al., 2008).
b. Complicated urinary tract infection, including pyelonephritis
Naber et al. (2007) conducted a multicenter double-blind randomized study of doripenem (500 mg every 8 hours, over 1 hour) versus 522 Carbapenems levofloxacin (250 mg every 24 hours, over 1 hour) for adults with complicated urinary tract infections, including pyelonephritis.
c. Hospital-acquired pneumonia, including ventilator-associated pneumonia
Two randomized trials of doripenem in the treatment of hospitalacquired pneumonia have been performed. Doripenem has been compared with piperacillin–tazobactam in the treatment of adults with hospital-acquired pneumonia, specifically nonventilated patients and those ventilated for fewer than 5 days (Rea-Neto et al., 2008). In general terms, critically ill and immunocompromised patients were excluded from this study.
References
Andes DR, Kiem S, Craig WA (2003b). In-vivo pharmacodynamic activity of a
new carbapenem, doripenem (DOR), against multiple bacteria in a murine
thigh infection model. Program and abstracts of the 43th Interscience
Conference on Antimicrobial Agents and Chemotherapy, Chicago, IL.
American Society for Microbiology (Abstract A-308).
Bhavnani SM, Hammel JP, Cirincione BB et al. (2005). Use of pharmacokineticpharmacodynamic
target attainment analyses to support phase 2 and 3
dosing strategies for doripenem. Antimicrob Agents Chemother 49: 3944.
Brown SD, Traczewski MM (2005). Comparative in vitro antimicrobial activity
of a new carbapenem, doripenem: tentative disc diffusion criteria and quality
control. J Antimicrob Chemother 55: 944.
Chastre JR, Wunderink R, Prokoclmer P et al. (2008). Efficacy and safety of
intravenous infusion of doripenem versus imipenem in ventilator-associated
pneumonia: a multicenter, randomized study. Crit Care Med 36: 1089.
Chen YE, Garber E, Zhao Q et al. (2005). In vitro activity of doripenem (S-
4661) against multidrug-resistant gram-negative bacilli isolated from patients
with cystic fibrosis. Antimicrob Agents Chemother 49: 2510.
Davies TA, Shang W, Bush K et al. (2008). Affinity of doripenem and
comparators to penicillin-binding proteins in Escherichia coli and
Pseudomonas aeruginosa. Antimicrob Agents Chemother 52: 1510.
Endimiani A, Hujer AM, Perez F et al. (2009). Characterization of blaKPCcontaining
Klebsiella pneumoniae isolates detected in different institutions in
the Eastern USA. J Antimicrob Chemother 63: 427.
Fink MP, Snydman DR, Niederman MS et al. (1994). Treatment of severe
pneumonia in hospitalized patients: Results of a multicenter, randomized,
double-blind trial comparing intravenous ciprofloxacin with imipenemcilastatin.
The Severe Pneumonia Study Group. Antimicrob Agents
Chemother 38: 547.
Ge Y, Wikler MA, Sahm DF et al. (2004). In vitro antimicrobial activity of
doripenem, a new carbapenem. Antimicrob Agents Chemother 48: 1384.
Horiuchi M, Kimura M, Tokumura M et al. (2006). Absence of convulsive
liability of doripenem, a new carbapenem antibiotic, in comparison with
beta-lactam antibiotics. Toxicology 222: 114.
Ikawa K, Morikawa N, Urakawa N et al. (2007). Peritoneal penetration of
doripenem after intravenous administration in abdominal-surgery patients. J
Antimicrob Chemother 60: 1395.
Iso Y, Irie T, Iwaki Tet al. (1996). A novel 1 beta-methylcarbapenem antibiotic,
S-4661. Synthesis and structure-activity relationships of 2-(5-substituted
pyrrolidin-3-ylthio)-1 beta-methylcarbapenems. J Antibiot (Tokyo) 49: 199.
Jones RN, Sader HS, Fritsche TR (2005). Comparative activity of doripenem and
three other carbapenems tested against Gram-negative bacilli with various
beta-lactamase resistance mechanisms. Diagn Microbiol Infect Dis 52: 71.
Katsube T, Yamano Y, Yano Y et al. (2008). Pharmacokinetic-pharmacodynamic
modeling and simulation for in vivo bactericidal effect in murine infection
model. J Pharm Sci 97: 1606.
You may like
Lastest Price from Doripenem manufacturers
US $0.00/kg2024-04-29
- CAS:
- 148016-81-3
- Min. Order:
- 1kg
- Purity:
- 99%
- Supply Ability:
- 20tons

US $0.00/kg2024-04-12
- CAS:
- 148016-81-3
- Min. Order:
- 1kg
- Purity:
- 99%
- Supply Ability:
- 2000ton