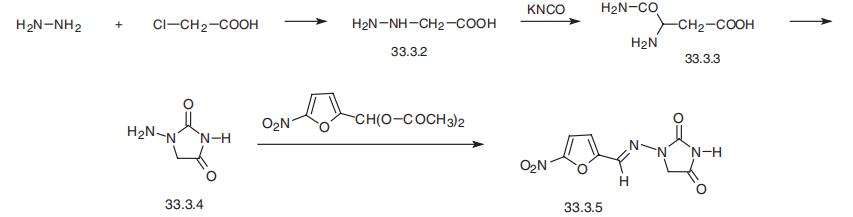
Nitrofurantoin
- Product NameNitrofurantoin
- CAS67-20-9
- CBNumberCB7346080
- MFC8H6N4O5
- MW238.16
- EINECS200-646-5
- MDL NumberMFCD00003224
- MOL File67-20-9.mol
- MSDS FileSDS
Chemical Properties
| Melting point | 268°C |
| Boiling point | 380.75°C (rough estimate) |
| Density | 1.5824 (rough estimate) |
| refractive index | 1.6700 (estimate) |
| storage temp. | Keep in dark place,Inert atmosphere,Room temperature |
| solubility | DMF: soluble50mg/mL |
| pka | 7.2(at 25℃) |
| form | crystalline |
| color | yellow |
| Water Solubility | <0.01 g/100 mL at 19 ºC |
| Sensitive | Light Sensitive & Hygroscopic |
| λmax | 358nm(MeOH)(lit.) |
| Merck | 14,6599 |
| BRN | 893207 |
| BCS Class | 2 |
| Stability | Stability Stable, but light-sensitive. Combustible. Incompatible with strong oxidizing agents, strong alkalies, strong acids. Decomposes upon contact with most metals other than stainless steel and aluminium. |
| InChI | 1S/C8H6N4O5/c13-6-4-11(8(14)10-6)9-3-5-1-2-7(17-5)12(15)16/h1-3H,4H2,(H,10,13,14)/b9-3+ |
| InChIKey | NXFQHRVNIOXGAQ-YCRREMRBSA-N |
Safety
| Symbol(GHS) |
 
|
|||||||||
| Signal word | Danger | |||||||||
| Hazard statements | H302-H317-H334 | |||||||||
| Precautionary statements | P261-P264-P280-P301+P312-P302+P352-P304+P340+P312 | |||||||||
| Hazard Codes | Xn | |||||||||
| Risk Statements | 22-42/43 | |||||||||
| Safety Statements | 22-36/37-45 | |||||||||
| RIDADR | 2811 | |||||||||
| WGK Germany | 3 | |||||||||
| RTECS | MU2800000 | |||||||||
| TSCA | TSCA listed | |||||||||
| HazardClass | 6.1(b) | |||||||||
| PackingGroup | III | |||||||||
| HS Code | 29349990 | |||||||||
| Storage Class | 11 - Combustible Solids | |||||||||
| Hazard Classifications | Acute Tox. 4 Oral Resp. Sens. 1 Skin Sens. 1 | |||||||||
| Hazardous Substances Data | 67-20-9(Hazardous Substances Data) | |||||||||
| Toxicity | LD50 oral in rat: 604mg/kg | |||||||||
| NFPA 704: |
|